
Disclaimer: this resource is intended for speech and language therapists and students of this profession. If you require therapy for aphasia please contact a speech and language therapist.
Visual Action Therapy (VAT)
Summary: Visual Action Therapy (VAT) is a structured, non-verbal approach for clients with global or near-global aphasia and limb/oral ideomotor apraxia that teaches the use of symbolic gestures in communication (e.g. making a peeling motion to indicate ¨banana¨) (Helm-Estabrooks, Albert, & Nicholas, 2014). In pure VAT the therapist uses no spoken communication during tasks, with all instructions and reinforcements being non-verbal.
Criteria for Treatment: Clients who may benefit from VAT are those who have:
(Helm-Estabrooks et al., 2014)
- Experienced a left hemisphere stroke and display global (or near-global) aphasia
- Moderate to severe limb and oral apraxia
- Moderately preserved visual perception and memory abilities
- Some spontaneous gestures during interactions (e.g. waving goodbye)
- Good alertness, attention, and motivation
(Helm-Estabrooks et al., 2014)
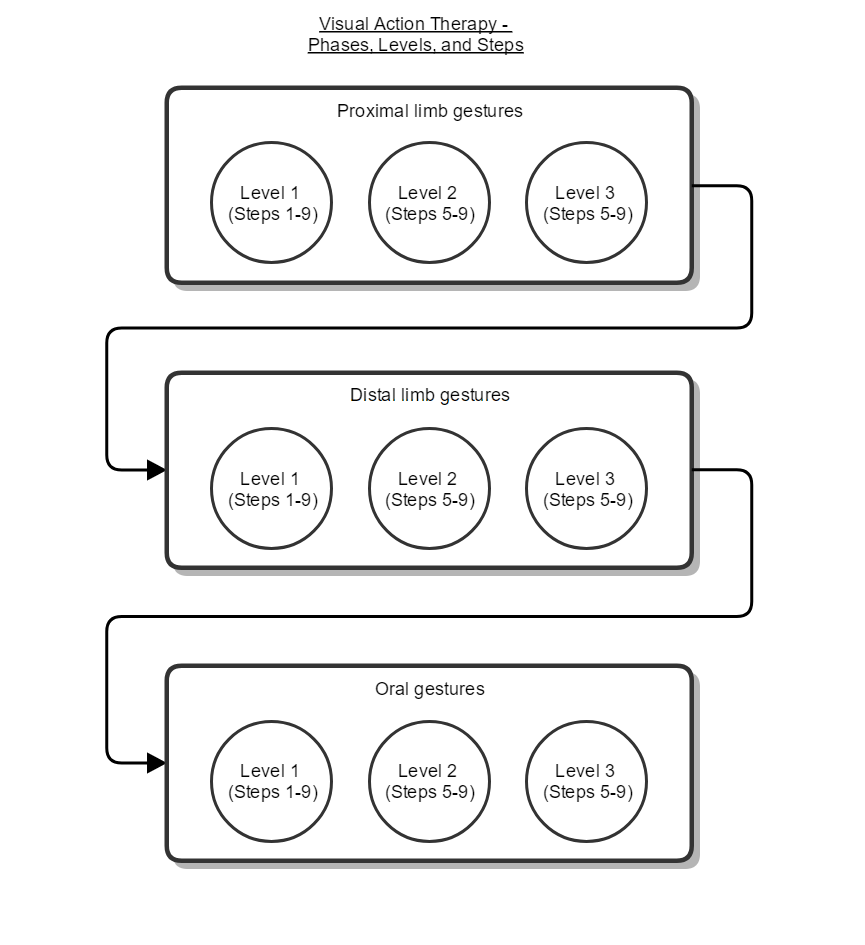
Example: VAT is divided into 3 broad phases (see diagram, below). Treatment starts with proximal limb gestures (i.e. gross movements such as miming the use of a hammer) before moving on to distal limb gestures (i.e. hand and finger movements such as miming turning a key) and, finally, oral gestures (e.g. the movement produced when miming use of lipstick or brushing teeth). 5 gestures are targeted within each of these phases.
Each phase of VAT is further divided into 3 levels (see diagram, below). Progress through these levels requires the client to understand (i.e. associate objects and pictures with target gestures) and be able to use these target gestures to non-verbally request the corresponding objects.
Each phase of VAT is further divided into 3 levels (see diagram, below). Progress through these levels requires the client to understand (i.e. associate objects and pictures with target gestures) and be able to use these target gestures to non-verbally request the corresponding objects.
- Level 1: steps 1-9 are carried out using objects, drawings of the objects, and drawings of a figure using each of the objects. Contextual props may be used during steps 2-4 to further illustrate and practise the appropriate use of real objects (e.g. a screw in wood to allow the client to practise using a screwdriver appropriately).
- Level 2: steps 5-9 are carried out again as in level 1, except that action pictures are used in place of the real object (i.e. no real objects are used during these steps.)
- Level 3: steps 5-9 are carried out again as in level 2, except that line drawings are used in place of the action pictures.
Scoring criteria:
For each scored step (i.e. steps : 1a, 1b, 1c, 1d, 2, 4, 6, 7, & 9):
Clients must score at least 4.5 (out of a possible 5) in each scored step to progress to the next.
Procedure for administering steps:
Below are detailed the steps in level 1. Levels 2 & 3 comprise only steps 5-9 and use different resources, i.e. action or line drawings in place of real objects, see above for details. The therapist should offer support as required (e.g. modelling of responses or hand-over-hand support to produce gestures).
Once steps 1-9 are complete in level 1, move on to level 2 and, finally, level 3 (details above).
For details on the delivery of VAT, as well as stimulus pictures and score sheets for recording clients’ progress through the phases, see Helm-Estabrooks et al. (2014).
For each scored step (i.e. steps : 1a, 1b, 1c, 1d, 2, 4, 6, 7, & 9):
- Correct responses with no groping or notable hesitation receive 1 point
- Responses which are delayed or which the client self-corrects receive a half point
- All other responses are scored 0
Clients must score at least 4.5 (out of a possible 5) in each scored step to progress to the next.
Procedure for administering steps:
Below are detailed the steps in level 1. Levels 2 & 3 comprise only steps 5-9 and use different resources, i.e. action or line drawings in place of real objects, see above for details. The therapist should offer support as required (e.g. modelling of responses or hand-over-hand support to produce gestures).
- Step 1 is divided into 4 stages (a-d) and targets the client’s ability to match objects with drawings.
- Step 1a) Placing objects on drawings: The therapist places the 5 line drawings on a table in front of the client, arranged in a random order. The client is then handed an object that matches one of the drawings. The client is required to place the object on top of the corresponding drawing. The object/drawing pairs are left on the table once matched, resulting in decreasing difficulty as the task progresses. Repeat for all 5 objects. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 1b) Placing drawings on objects: The therapist places the 5 objects in front of the client. The client is handed each of the 5 line drawings one at a time and is required to place the drawing on top of the corresponding object. As above, the object/drawing pairs are left on the table once matched. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 1c) Pointing to objects in response to drawings: The therapist rearranges the objects in front of the client and holds up a line drawing that matches one of the objects. The client must point to, but not pick up, the corresponding object. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 1d) Pointing to drawings in response to objects: The therapist places the 5 line drawings in front of the client and then holds up an object that matches one of the drawings. The client must point to the corresponding drawing. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 1a) Placing objects on drawings: The therapist places the 5 line drawings on a table in front of the client, arranged in a random order. The client is then handed an object that matches one of the drawings. The client is required to place the object on top of the corresponding drawing. The object/drawing pairs are left on the table once matched, resulting in decreasing difficulty as the task progresses. Repeat for all 5 objects. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 2) Manipulating objects appropriately: This step targets the client’s ability to manipulate real objects in an appropriate fashion. The therapist first demonstrates the use of each object (e.g. picking up flag and waving it), then places the object in front of the client. The client is encouraged to pick up the object and demonstrate its use. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 3) Demonstration of action pictures: This step is designed to make the client aware that each of the action pictures should be understood as an instruction to pick up the corresponding real object and demonstrate its use. The therapist randomly chooses an object and its corresponding action picture. These are placed in front of the client. The therapist first points to the action picture and then picks up the object and demonstrates its use. The therapist repeats this step for all object/action picture pairs. This step is intended to orient the client and is not scored.
- Step 4) Demonstrating object use in response to action pictures: This step targets the client’s ability to choose a target object and demonstrate its use when shown the corresponding action picture. The therapist places the five objects in front of the client in a random order. The therapist then holds up an action picture and the client is encouraged to select and demonstrate the use of the corresponding object. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 5) Demonstration of link between gestures and visible objects: This step is designed to make the client aware that gestures can be used in place of real objects. The therapist places one of the objects in front of the client, at a short distance, and demonstrates the corresponding gesture. This step is repeated for each of the five target objects. The therapist should progress through these slowly to allow the client to make the link between the real object and its corresponding gesture. This step is intended to orient the client and is not scored.
- Step 6) Recognition of gestures: This step targets the client’s ability to match gestures with corresponding objects. The five target objects are placed in front of the client in a random order. The therapist then produces a gesture. The client is required to select the corresponding object. The client must score at least 4.5 out of 5 to progress to the next step.
- Step 7) Production of gestures: This step targets the client’s ability to produce gestures in response to seeing the corresponding objects. The therapist displays each of the five objects, one at a time. The client is required to produce the corresponding gesture. In order to score during these trials the client must produce the gesture without touching the objects. However, if the client struggles to produce the gestures, consider having them first perform the action whilst holding the associated object before gradually removing the object and prompting them to continue the gesture. The client must score at least 4.5 out of 5 to progress to the next step. Half-points are awarded for delayed responses and self-corrections.
- Step 8) Demonstration of link between gestures and hidden objects: This step is designed to make the client aware that gestures can be used to represent objects that are not currently visible. The therapist places 2 of the objects on the table, producing the corresponding gesture for each while doing so, before hiding both under a box. The therapist then removes one object and produces the gesture for the object that remains hidden under the box. This process is repeated so that all 5 objects are gestured whilst remaining hidden under the box. This step is intended to orient the client and is not scored.
- Step 9) Indicating hidden objects using gestures: The aim of this step is for the client to produce a gesture to signify a corresponding hidden object. The therapist places two objects on the table and the client is encouraged to produce the corresponding gestures for both of these objects. Then the therapist hides both objects under a box, waits 6 seconds, and removes one object. The client is then encouraged to produce the gesture for the remaining, hidden, object. This process is repeated so that all 5 objects are gestured whilst remaining hidden under the box. The client must score at least 4.5 out of 5 to progress to the next step.
Once steps 1-9 are complete in level 1, move on to level 2 and, finally, level 3 (details above).
For details on the delivery of VAT, as well as stimulus pictures and score sheets for recording clients’ progress through the phases, see Helm-Estabrooks et al. (2014).
Evidence Base: Helm-Estabrooks, Fitzpatrick, & Barresi (1982) delivered a VAT programme to 8 participants with global aphasia. Significant improvements were noted in the participants’ pantomimic and auditory comprehension skills as measuredon the Porch Index of Communicative Ability (PICA). No change was noted in participants’ verbal expression following treatment.
Hypothesising that bucco-facial apraxia may have prevented the participants in the 1982 study from making gains in verbal expression, Ramsberger & Helm-Estabrooks (1989) carried out an additional study using a form of VAT adapted to treat 6 participants with aphasia and moderate to severe bucco-facial apraxia. The gestures/pictures used in this programme were all associated with the mouth and face (e.g. razor, straw, and whistle). In addition to significant gains in the participants’ pantomimic and auditory comprehension skills (as in the 1982 study), word repetition ability was also found to improve significantly.
Conlon & McNeil (1991) examined the effects of VAT for 2 participants with global aphasia in a single-subject design. Participants were tested on both trained and untrained targets. Thirty sessions, each lasting fifty-five minutes, were delivered over a 7 week period. Results were largely consistent with the findings in Helm-Estabrooks et al.’s (1982) study. However, generalisation to untrained targets was noted to be ‘extremely poor’ for both participants.
Hypothesising that bucco-facial apraxia may have prevented the participants in the 1982 study from making gains in verbal expression, Ramsberger & Helm-Estabrooks (1989) carried out an additional study using a form of VAT adapted to treat 6 participants with aphasia and moderate to severe bucco-facial apraxia. The gestures/pictures used in this programme were all associated with the mouth and face (e.g. razor, straw, and whistle). In addition to significant gains in the participants’ pantomimic and auditory comprehension skills (as in the 1982 study), word repetition ability was also found to improve significantly.
Conlon & McNeil (1991) examined the effects of VAT for 2 participants with global aphasia in a single-subject design. Participants were tested on both trained and untrained targets. Thirty sessions, each lasting fifty-five minutes, were delivered over a 7 week period. Results were largely consistent with the findings in Helm-Estabrooks et al.’s (1982) study. However, generalisation to untrained targets was noted to be ‘extremely poor’ for both participants.
References
Conlon, C.P. & McNeil, M.R., 1991. The efficacy of treatment for two globally aphasic adults using Visual Action Therapy. In Clinical Aphasiology Conference: Clinical Aphasiology Conference (Lake Tahoe, NV). [online] Available at: <http://aphasiology.pitt.edu/archive/00000114/01/19-18.pdf>[Accessed 31/08//2016]
Helm-Estabrooks, N., Albert, M., & Nicholas, M., 2014. Manual of aphasia and aphasia therapy. 3rd ed. Austin, TX: PRO-ED
Helm-Estabrooks, N., Fitzpatrick, P.M., & Barresi, B., 1982. Visual Action Therapy for global aphasia. Journal of Speech and Hearing Disorders, 47(4), 385-389
Ramsberger, G. & Helm-Estabrooks, N., 1989. Visual Action Therapy for bucco-facial apraxia. In: Prescot, T. ed. Clinical aphasiology. Massachusetts: College-Hill, 395-406
Conlon, C.P. & McNeil, M.R., 1991. The efficacy of treatment for two globally aphasic adults using Visual Action Therapy. In Clinical Aphasiology Conference: Clinical Aphasiology Conference (Lake Tahoe, NV). [online] Available at: <http://aphasiology.pitt.edu/archive/00000114/01/19-18.pdf>[Accessed 31/08//2016]
Helm-Estabrooks, N., Albert, M., & Nicholas, M., 2014. Manual of aphasia and aphasia therapy. 3rd ed. Austin, TX: PRO-ED
Helm-Estabrooks, N., Fitzpatrick, P.M., & Barresi, B., 1982. Visual Action Therapy for global aphasia. Journal of Speech and Hearing Disorders, 47(4), 385-389
Ramsberger, G. & Helm-Estabrooks, N., 1989. Visual Action Therapy for bucco-facial apraxia. In: Prescot, T. ed. Clinical aphasiology. Massachusetts: College-Hill, 395-406
|
|

|
